Hypermobility &
Ehlers-Danlos Syndrome

What is hypermobility?
Hypermobility means that your joints are extra flexible. Some people refer to this as being “double jointed.” A medical professional, such as a physical therapist or orthopedic doctor may call it having “increased range of motion.” You can be hypermobile in one joint or in many joints. You may also be hypermobile at one point in your life and not another due to injury or increased stiffness. Hypermobility is actually common and can affect up to 20% of the general population. Being hypermobile in itself does not necessarily mean you have a health concern.
What is Generalized Joint Hypermobility?
Generalized Joint Hypermobility used to be called Joint Hypermobility Syndrome (JHS) or Benign Joint Hypermobility Syndrome (BJHS). In 2017, the name was changed to Generalized Joint Hypermobility (GJH). The current definition is based on the Beighton criteria (see video and/ or Criterion 1 of hEDS checklist in Resources section below). It essentially means that you have hypermobile joints all over your body. But you may notice that the Beighton score does not test all joints - in fact, it only tests 3 in the upper body (both sides), the spine, and the knees. Many hypermobility/ EDS experts agree that this criteria is inadequate and may miss some people with hypermobility. Dr. Jennifer Tang is part of the Norris Lab think tank to help determine new criteria for GJH, Hypermobile Spectrum Disorder (HSD) and Hypermobile Ehlers-Danlos Syndrome (hEDS). We expect to have a new definition of these conditions in 2026 and 2027.
What is Hypermobile Spectrum Disorder?
Hypermobile Spectrum Disorder (HSD) is defined by joint hypermobility that causes a disturbance of normal function. The most common symptoms of HSD are joint instability, joint pains, other musculoskeletal pains or injury, and chronic fatigue. Joint instability may manifest as subluxations (partial dislocations) or dislocations or frequent ankle rolls/ sprains. There is often overlap with dysautonomia and/ or Postural Orthostatic Tachycardia Syndrome (POTS), Mast Cell Activation Syndrome (MCAS), gastrointestinal dysfunction, autoimmune diseases, and headaches. While the definition of HSD is currently distinct from the definition for hypermobile Ehlers-Danlos Syndrome (hEDS), many experts feel that HSD and hEDS are actually along a spectrum of the same condition and that opinion is likely to be reflected in the updated definitions to come in 2026-2027.
What is Ehlers-Danlos Syndrome?
According to the EDS Society, there are 13 different types of Ehlers-Danlos Syndrome (EDS). The most common type is hypermobile EDS (hEDS), which affects approximately 1 in 3000-5000 people. It’s hard to know exactly how many people have EDS because there are many barriers to diagnosis, including lack of knowledge on the part of medical professionals, patients’ lack of access to a doctor who can diagnose EDS, and frequent misdiagnosis. Currently, there is no testable genetic marker for hEDS, so it is a clinical diagnosis (see hEDS checklist in Resources section below). This means that any medical professional can go through the checklist with you and diagnose you, though many are unfortunately not comfortable doing so due to lack of knowledge or experience. Researchers have identified potential genes (KLK15, TNXB) that may contribute to hEDS, but these account for only a small percentage of cases. Most experts believe that illness with hEDS occurs when those with a genetic predisposition face environmental triggers, such as infection, stress, trauma, hormonal changes, or environmental toxins. As stated above, HSD and hEDS share similar characteristics and are likely to represent differing manifestations of the same illness. The hEDS “pentad” refers to a group of five conditions that frequently coexist. It includes hEDS, dysautonomia (such as POTS), Mast Cell Activation Syndrome (MCAS), gastrointestinal dysfunction, and autoimmune disease.
The other 12 types of EDS are all diagnosed by genetic markers. Classical EDS (cEDS) occurs in about 1 in 20,000-40,000 people and is caused by a mutation in the COL5A1, COL5A2, or COL1A1 genes, which affect type V or type I collagen. It is inherited in an autosomal dominant manner, which means that if one parent has the gene and passes it onto their child, their child may manifest cEDS by having just one copy of the gene mutation. Common symptoms of cEDS are very stretchy, fragile skin that bruises easily, scars that are indented/ sunken (atrophic), along with joint hypermobility and instability.
Vascular EDS (vEDS) affects about 1 in 100,000 -200,000 people. It is inherited in an autosomal dominant pattern and due to a genetic mutation in COL3A1 or COL1A1 genes that code for type III and type I collagen. vEDS can cause life threatening complications such as arterial aneurysm, dissection, and rupture, particularly before age 40. Those with vEDS may also experience bowel perforation (hole in intestines), pneumothorax (collapsed lung), or uterine rupture in 3rd trimester of pregnancy.
The other EDS types are very rare, occurring in about 1 in 1 million people. Some are autosomal dominant and others are autosomal recessive, meaning you need to inherit 2 copies of the mutated gene (one from each parent) to be affected. This is a list of the other EDS types:
Periodontal
Kyphoscoliotic
Spondylodysplastic
Arthrochalasia
Musculocontractural
Classical-like
Dermatosparaxis
Myopathic
Cardiovalvular
Brittle Cornea Syndrome
How do I know if I need genetic testing?
A knowledgeable medical professional will go over your personal medical history, your family’s medical history, and do a thorough examination to determine (1) if you meet criteria for hypermobile EDS (hEDS), and (2) whether classical EDS (cEDS), vascular EDS (vEDS), or the other rarer EDS types are suspected. Remember, hEDS is the most common type. If you meet criteria for hEDS, and have no clues that point to the other types, you do not necessarily need genetic testing.
How can I get diagnosed and treated for Hypermobility, HSD, or EDS?
Unfortunately, because of lack of knowledge by medical professionals, many people with hypermobility have gone many years and even decades without getting answers to their health concerns. If you suspect that you have health issues related to hypermobility - chronic pains, joint instability, musculoskeletal injuries, chronic fatigue, gut dysfunction - book an appointment with Dr. Jennifer Tang for an evaluation in California.
Resources for hypermobility and EDS
How is Generalized Joint Hypermobility (GJH) diagnosed? Understanding the Beighton Score.
Watch a clinical demostration of the Beighton score - the standard 9 point system to measure joint hypermobility. This video walks through the specific assessments for the pinky fingers, thumbs, elbows, knees, and spine.
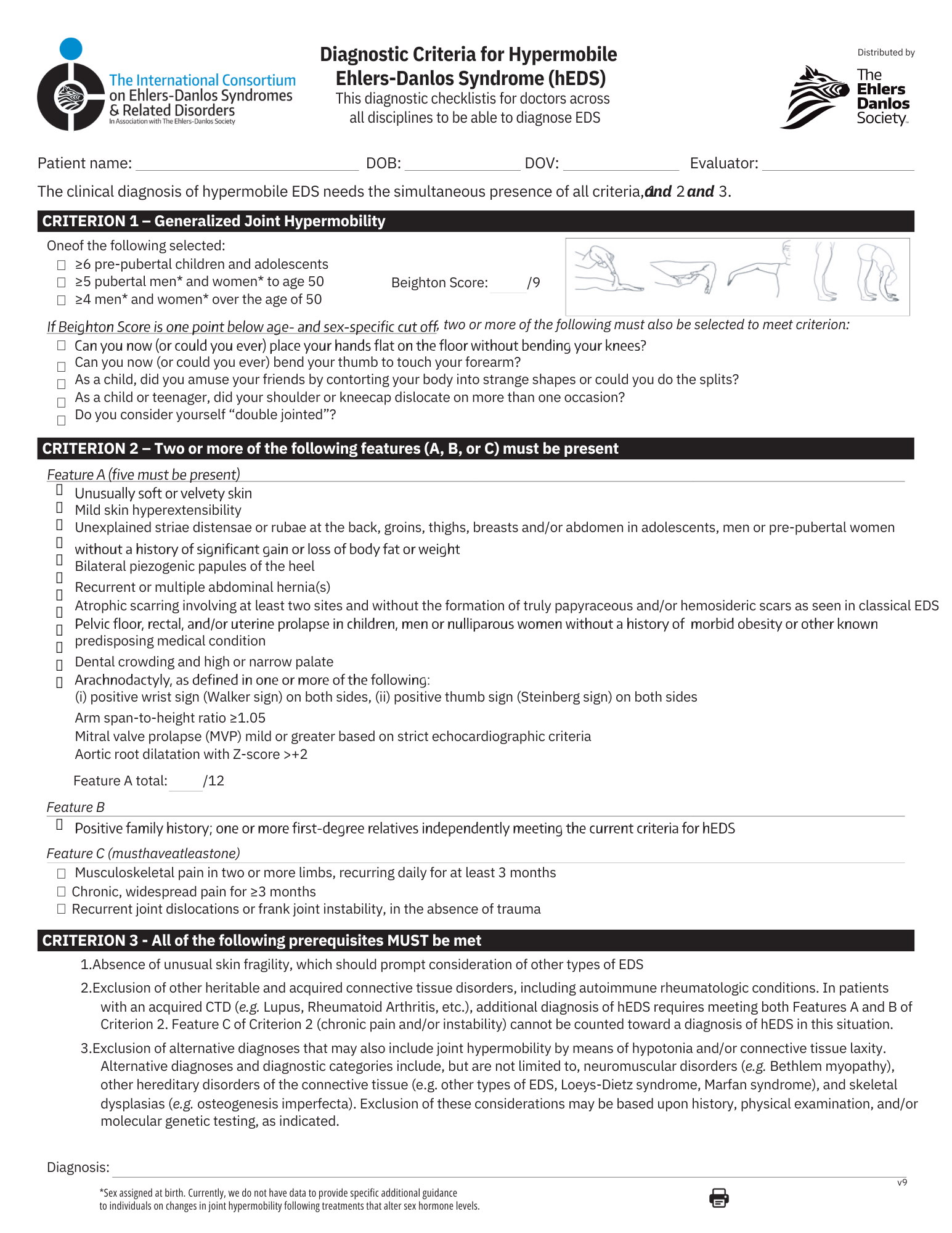
Diagnostic criteria for Hypermobile EDS
Click here to download printable version
Online Links
Dr. Jennifer Tang listing on EDS Society Website
Ehlers- Danlos Society
The Norris Lab
A leader in EDS genetic research
UW Health EDS/ HSD Clinical guidelines
Books
Disjointed, Edited by Diana Jovin
A Guide to Living with Ehlers-Danlos Syndrome by Isobel Knight
Living Life to the Fullest with EDS by Kevin and Kathleen Muldowney (Physical therapists)